Have you ever noticed bright red blood on the toilet paper or felt a strange lump near your anus? You are not alone. In fact, about 75% of adults will deal with hemorrhoids at some point in their lives. It is a common issue, yet many people suffer in silence due to embarrassment. Understanding whether you have internal or external hemorrhoids is the first step toward getting relief. The good news is that most cases can be managed effectively with simple lifestyle changes or minor procedures.
What Are Hemorrhoids?
To understand hemorrhoids, you need to know a bit about anatomy. Hemorrhoids are simply swollen veins in your lower rectum and anus. Think of them like varicose veins, but located in a very sensitive area. Everyone has these vascular cushions; they help control stool release. They become a problem when pressure causes them to swell, stretch, or irritate.
This condition isn't new. Medical records from the Ebers Papyrus in 1550 BCE mention it. However, modern classification was established by French surgeon Auguste Nélaton in the 19th century. Today, doctors classify hemorrhoids based on where they form and how severe they are. The location determines your symptoms and the best treatment path.
Internal vs. External Hemorrhoids: Key Differences
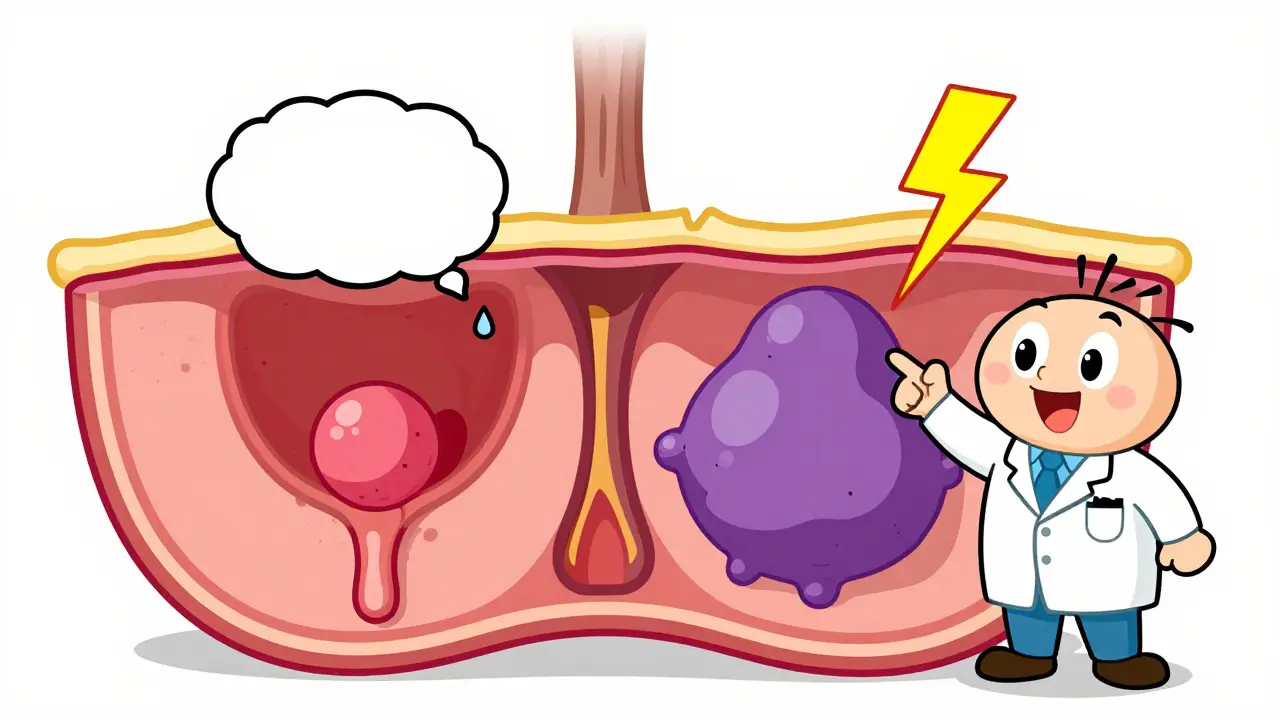
The main difference lies in their location relative to the dentate line (the border inside the anal canal). This anatomical detail explains why one type hurts more than the other.
| Feature | Internal Hemorrhoids | External Hemorrhoids |
|---|---|---|
| Location | Above the dentate line, inside the rectum | Below the dentate line, under the skin around the anus |
| Pain Sensitivity | Low (covered by mucosa with few pain receptors) | High (rich in pain-sensitive nerve endings) |
| Primary Symptom | Painless bright red bleeding | Itching, swelling, pain, visible lumps |
| Visibility | Usually invisible unless prolapsed | Visible as skin-colored or purple lumps |
| Complication Risk | Prolapse, anemia from chronic bleeding | Thrombosis (blood clot formation) |
Internal Hemorrhoids
Internal hemorrhoids form inside the rectum. Because this area lacks significant pain nerves, you might not feel them at all. Instead, the warning sign is often painless rectal bleeding. You may see bright red blood on the toilet paper, in the bowl, or streaked on your stool. While this looks alarming, it is usually not dangerous if caused by hemorrhoids. However, you should never assume bleeding is just hemorrhoids without a doctor's check-up, as it can signal other conditions like colorectal cancer or inflammatory bowel disease.
Doctors grade internal hemorrhoids from I to IV based on severity:
- Grade I: Bleeding occurs, but no tissue protrudes.
- Grade II: Tissue prolapses (comes out) during straining but goes back in on its own.
- Grade III: Tissue prolapses and must be pushed back in manually.
- Grade IV: Tissue is permanently prolapsed and cannot be pushed back.
External Hemorrhoids
External hemorrhoids develop under the skin surrounding the anus. This area is packed with nerve endings, making these hemorrhoids much more painful. You might feel itching, swelling, or a tender lump. Sitting can become extremely uncomfortable. If a blood clot forms inside an external hemorrhoid, it becomes thrombosed. A thrombosed hemorrhoid appears as a firm, purple or blue lump and causes sudden, severe pain. This requires prompt medical attention for relief.
Common Causes and Risk Factors
Hemorrhoids result from increased pressure on the veins in your pelvic and rectal area. Several daily habits contribute to this pressure:
- Straining during bowel movements: Chronic constipation forces you to push harder, increasing vein pressure.
- Prolonged sitting on the toilet: Spending too much time on the toilet (especially looking at your phone) keeps pressure on the rectal veins.
- Low-fiber diet: Lack of fiber leads to hard stools and straining.
- Obesity: Extra weight increases abdominal pressure.
- Pregnancy: About 25-35% of pregnant women develop hemorrhoids due to hormonal changes and pressure from the growing uterus.
- Heavy lifting: Regular heavy lifting strains the pelvic floor.
Treatment Options for Mild Cases
Most mild hemorrhoids improve with home care. The goal is to reduce pressure and soothe irritation.
- Increase Fiber Intake: Aim for 25-30 grams of fiber daily. Foods like oats, beans, fruits, and vegetables soften stool and make it easier to pass.
- Stay Hydrated: Drink 8-10 glasses of water daily. Fiber works best when combined with plenty of fluids.
- Sitz Baths: Soak your anal area in warm water for 15-20 minutes, 2-3 times a day. This reduces swelling and relaxes muscles.
- Over-the-Counter Remedies: Hydrocortisone creams or witch hazel pads can relieve itching and inflammation temporarily.
- Improve Toilet Habits: Limit toilet time to 5 minutes. Use a small footstool to elevate your knees above your hips. This position straightens the rectal angle and reduces straining by up to 30%.
Medical Procedures for Severe Cases
If home remedies don't work, or if you have Grade II-IV internal hemorrhoids or thrombosed external hemorrhoids, a doctor may recommend a procedure.
Minimally Invasive Treatments
These are typically done in a doctor's office with little downtime.
- Rubber Band Ligation: A small rubber band is placed around the base of an internal hemorrhoid to cut off its blood supply. It falls off within a week. This is 90% effective for Grades I-III.
- Sclerotherapy: A chemical solution is injected into the hemorrhoid to shrink it.
- Infrared Coagulation: Heat is used to scar and shrink the hemorrhoid tissue.
Surgical Options
For severe or recurrent cases, surgery might be necessary.
- Hemorrhoidectomy: Surgical removal of the hemorrhoid. It has a 95% success rate but involves significant post-operative pain and a 2-4 week recovery period.
- Stapled Hemorrhoidopexy: This procedure repositions prolapsed tissue rather than removing it. It is less painful than traditional hemorrhoidectomy but has a higher recurrence rate.
- Incision and Clot Removal: For thrombosed external hemorrhoids, a doctor may make a small cut to remove the clot. This provides immediate pain relief if done within 72 hours of symptom onset.

When to See a Doctor
While hemorrhoids are common, self-diagnosis can be risky. You should consult a healthcare provider if you experience:
- Rectal bleeding that persists despite home treatment.
- Severe pain or discomfort that interferes with daily activities.
- Dizziness or lightheadedness, which could indicate significant blood loss.
- Changes in bowel habits or stool color (black or tarry stools).
- A lump that does not go away or worsens.
Remember, rectal bleeding can also be a sign of anal fissures, polyps, or colorectal cancer. A proper diagnosis ensures you get the right treatment. Don't let embarrassment delay care-doctors see this every day.
Prevention Strategies
Preventing hemorrhoids is largely about managing pressure in your rectal area. Here are practical tips:
- Eat a high-fiber diet consistently.
- Exercise regularly to promote healthy digestion.
- Go to the bathroom as soon as you feel the urge. Holding it in makes stool harder.
- Avoid straining. If nothing happens after a few minutes, get up and try later.
- Maintain a healthy weight to reduce abdominal pressure.
By adopting these habits, you can significantly reduce your risk of developing hemorrhoids or prevent recurrence after treatment. The American Society of Colon and Rectal Surgeons notes that adherence to these lifestyle changes lowers recurrence rates to 5-10%, compared to 50% for those who do not follow preventive measures.
Do internal hemorrhoids hurt?
Typically, no. Internal hemorrhoids are located above the dentate line where there are few pain receptors. They usually cause painless bleeding. However, if they prolapse (protrude) and become strangulated or thrombosed, they can cause significant pain.
How long does it take for hemorrhoids to go away?
Small external hemorrhoids may resolve in a few days with home treatment. Larger ones or internal hemorrhoids might take longer. Thrombosed external hemorrhoids can take 2-3 weeks for the pain to subside and the clot to dissolve or be removed.
Can hemorrhoids go away on their own?
Yes, mild hemorrhoids often improve with lifestyle changes like increased fiber intake and sitz baths. However, larger or prolapsed hemorrhoids usually require medical intervention to shrink or remove.
Is rectal bleeding always from hemorrhoids?
No. While hemorrhoids are a common cause, rectal bleeding can also result from anal fissures, diverticulitis, inflammatory bowel disease, or colorectal cancer. Always consult a doctor to rule out serious conditions.
Are hemorrhoids hereditary?
There is no direct genetic link causing hemorrhoids. However, you may inherit weaker vein walls or connective tissue, which can make you more susceptible to developing them under pressure.